
Genesis Life Care
Better Care Starts Here. Compassionate, personalized nursing home and senior care across Klang Valley & Johor Bahru.
Find the Right Care for Your Loved One
Our care advisors will get back to you within 24 hours.
No obligations. 100% confidential.
Comprehensive Care for Every Need
From long-term residential nursing to specialised memory care, we have the right support for your family.
Nursing Home Care
24/7 professional nursing care in a warm, homelike environment. Personalised care plans for each resident.
Learn more →Dementia & Memory Care
Specialised programmes for Alzheimer's, dementia, and Parkinson's. Safe, structured, and stimulating environment.
Learn more →Post-Operative Recovery
Short-term rehabilitation and recovery care after surgery. Physiotherapy and medical supervision included.
Learn more →Stroke Rehabilitation
Comprehensive stroke recovery with physiotherapy, occupational therapy, and 24-hour nursing support.
Learn more →Senior Day Care
Daytime care programmes with meals, activities, and supervision — ideal for families who need support during working hours.
Learn more →Respite Care
Short-term stays from a few days to several weeks — giving family caregivers a well-deserved break while their loved one receives full-service care.
Learn more →Nursing Home Cost Calculator
Get an instant personalised estimate based on the care your loved one needs. Select a centre, room type, care level, and add-on services — see the monthly cost breakdown in seconds.
No sign-up required. Estimates are indicative — final pricing confirmed after assessment.
Choose Your Centre
Compare pricing across our 5 centres in PJ, Klang, Kajang, Puchong & JB.
Customise Care Needs
Select room type, feeding assistance, wound care, rehab, dementia care & more.
See Your Estimate Instantly
Transparent monthly breakdown with no hidden costs. Starts from RM 2,500/month.
Why Families Trust Genesis Life Care
With over a decade of experience in elderly care, we combine medical expertise with genuine compassion. Every family receives personalised attention from our dedicated team of nurses and caregivers.

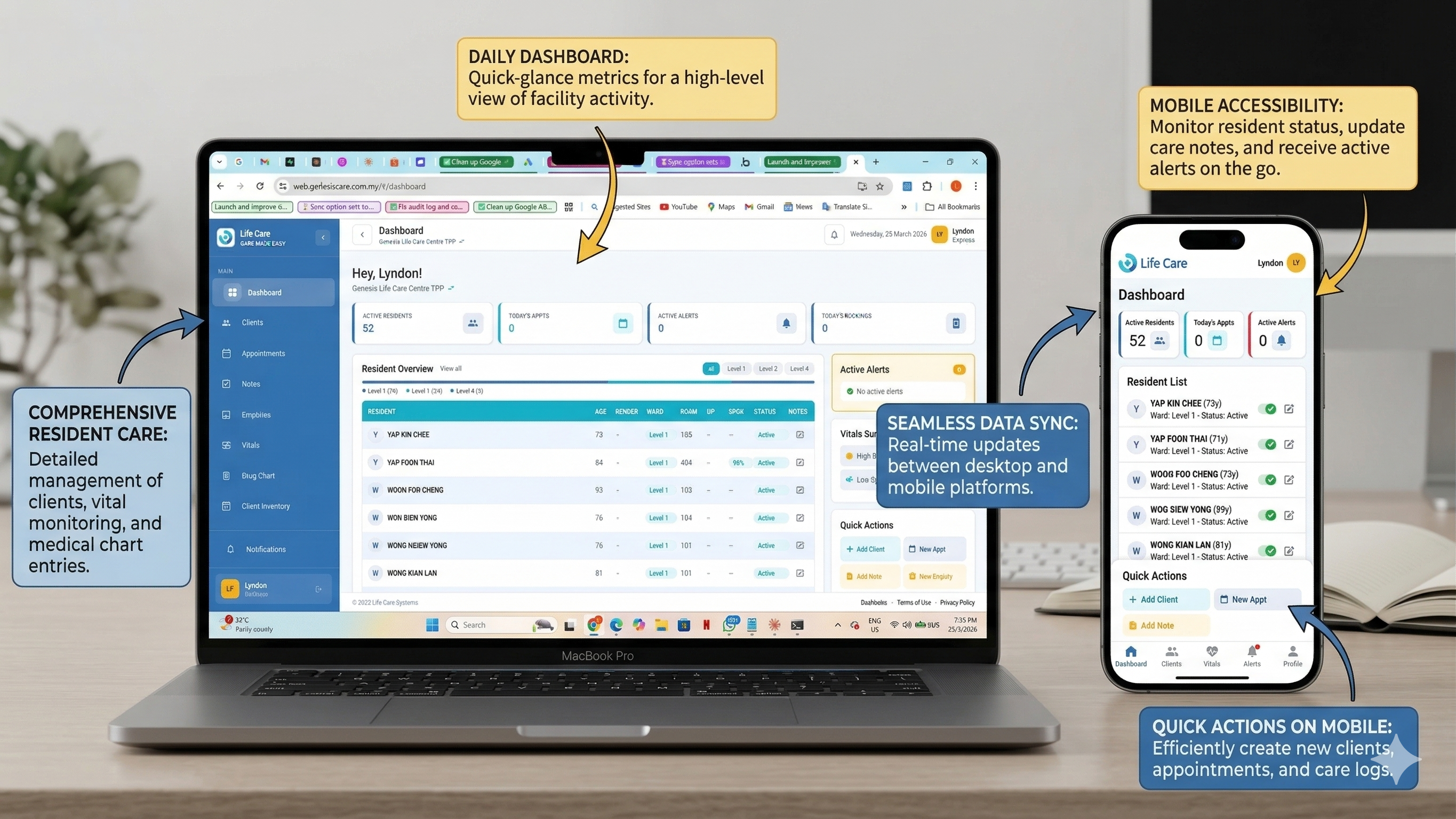
Malaysia's First AI-Powered Care Facility
Genesis Life Care is pioneering the use of artificial intelligence in Malaysia's aged care sector. Our proprietary technology platform harnesses AI to deliver safer, more comprehensive, and more affordable care — setting a new standard for what families can expect from a nursing home.
5 Centres Across Malaysia
Conveniently located across Klang Valley and Johor Bahru.



Hire a Trained Domestic Helper for Home Care
Through Agensi Pekerjaan GLC, we recruit and train domestic helpers from Indonesia and the Philippines specifically in elderly care and home nursing. Each helper undergoes our in-house training programme at Genesis Life Care before being placed with your family — so they arrive ready to provide professional, compassionate care from day one.
How It Works
Latest News & Guides
Home Care vs Nursing Home: Which Is Right for Your Elderly Parent in Malaysia?
Every family reaches a crossroads when caring for an ageing parent. Should your loved one receive care at home, or would a nursing home provide better quality of life? This guide helps you decide.

Best Elderly Care Centres in Johor Bahru
A guide to the best elderly care centres in Johor Bahru for families seeking quality nursing home services in southern Malaysia.
10 March 2026

Best Nursing Homes in KL & Selangor (2026)
A curated guide to the best nursing homes in Kuala Lumpur and Selangor for 2026, including ratings, services, and what makes each centre stand out.
10 March 2026
Frequently Asked Questions
How much does a nursing home cost in Malaysia?
Where are Genesis Life Care centres located?
What types of care does Genesis Life Care provide?
Is Genesis Life Care government-approved?
Can I visit a Genesis Life Care centre before making a decision?
Still have questions?
Our care advisors are happy to help. Speak to us directly or schedule a free visit to any of our centres.

Ready to Take the Next Step?
Contact us today for a free consultation. Our care advisors speak to dozens of families every week and can help find the perfect care solution for your loved one.